
National Conference Menstrual Health Drive
Questions? Please reach out to women@apamsa.org.
Response to the Fatal Shootings of Renee Good and Alex Pretti
On January 7, 2026, Immigration and Customs Enforcement (ICE) agents fatally shot Renee Good, a 37-year-old U.S. citizen, during an immigration raid in Minneapolis. A nearby physician was restricted from administering life support immediately after the shooting. Weeks later, on January 24, 2026, ICE agents in Minneapolis brutally murdered a second U.S. citizen, Alex Pretti, who was a 37-year-old ICU nurse attempting to help a civilian who had been pepper-sprayed. These deaths have occurred in the backdrop of at least 30 other deaths at ICE detention centers since the beginning of the Trump administration.
As students in the healthcare profession, we are frustrated by the blatant disregard for life in these encounters, as medical professionals are barred from providing emergency care for the communities they serve. Unrelenting immigration raids have prompted a public health emergency, as many immigrants have become too fearful to step outside their homes to seek medical care at hospitals that were once protected spaces.
Immigration enforcement raids have rattled the nation with indiscriminate investigations, deportations, and detention, often relying on racial profiling to target communities of color. A recent Supreme Court order (Noem v. Vasquez Perdomo) will condone investigations based on subjective assessments, such as skin tone or accented speech, allowing the U.S. Government to continue race-based searches if they meet “reasonable suspicion.”
National APAMSA strongly condemns the tragic killing of both Renee Good and Alex Pretti by ICE and is deeply concerned about federal officials’ lethal weaponization of immigration enforcement. APAMSA stands firmly against any form of violence and reaffirms its commitment to protect human lives, regardless of immigration status or background. We mourn the loss of Renee Good and Alex Pretti and extend our condolences to their family, friends, and community members affected by these tragedies.
We call for increased scrutiny of federal immigrant official deployment and practices and a full, unbiased investigation into these shootings. Furthermore, we urge comprehensive training for all law enforcement agents to de-escalate encounters and prevent the loss of innocent lives.
For questions regarding this statement, please contact the Rapid Response Director, Brian Leung at rapidresponse@apamsa.org

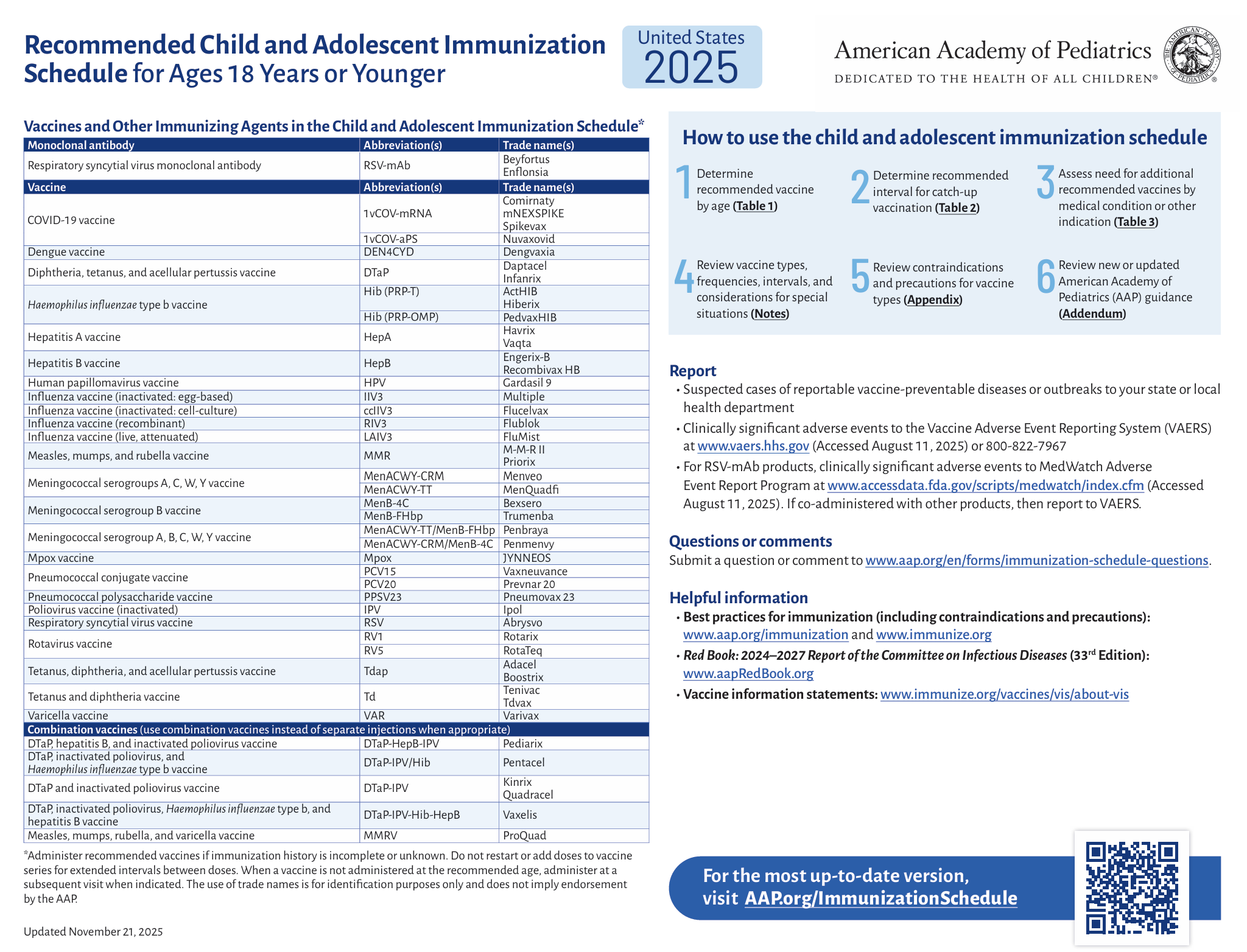
APAMSA x NCAPIP: Joint Statement on New Childhood Immunization Schedule
On January 5, 2026, the Centers for Disease Control and Prevention (CDC) unveiled a new childhood immunization schedule that has now curtailed the number of recommended vaccinations for children from 17 diseases to 11 diseases. Exactly one month after a presidential memorandum was issued to reexamine childhood immunization schedules, the CDC no longer recommends routine immunization with Hepatitis A, Hepatitis B, Influenza, Respiratory Syncytial Virus (RSV), Rotavirus, Meningococcal, and COVID-19. Instead, these vaccinations will be based on “Shared Clinical Decision-making” between parents and physicians, despite long-standing evidence of their benefits in protecting children’s lives. Hepatitis B, which affects a disproportionate portion of the AANHPI population, will no longer be universally recommended at birth according to new CDC guidelines.
APAMSA and NCAPIP are deeply concerned about the abrupt changes in the CDC’s childhood immunization schedule, made without public input or a rigorous scientific examination of the risks and benefits. These decisions may further erode trust in public health agencies and increase vaccination hesitancy. Recent research has already shown a decline in childhood vaccinations such as Mumps-Measles-Rubella, leading to outbreaks of measles across the nation.
As mentioned in a previous statement and in our policy compendium, we remain committed to advocating for universal Hepatitis B vaccinations and other necessary childhood immunizations. We urge policymakers at public health institutions to reconsider these changes and focus on evidence-based guidelines that match the United States population and its risks, rather than mirroring other countries’ individualized vaccination schedules.
Resources:
The American Academy of Pediatrics now maintains its own immunization schedule following the replacement of all members on the Advisory Committee on Immunization Practice (ACIP) by the US Secretary of Health and Human Services, Robert F. Kennedy Jr., last year.
For questions regarding this statement, please contact the Rapid Response Director, Brian Leung at rapidresponse@apamsa.org

More Op-Eds Coming Soon!
The APAMSA Op-Ed Series provides members with an accessible platform to share perspectives on medicine, advocacy, identity, and health equity. This initiative is designed to lower barriers to publication by offering clear submission guidelines, editorial support, and opportunities for mentorship throughout the writing process.
Op-eds may be written by national board members or general APAMSA members and are intended to amplify diverse voices while producing a polished, publishable piece. Selected submissions may be featured on the APAMSA website and shared through organizational channels, allowing contributors to engage meaningfully with APAMSA while gaining a tangible scholarly and advocacy-related product for their CVs.
Stay tuned for new op-ed pieces coming soon!
Leadership and Membership Transition
CHAPTER LEADERSHIP AND MEMBERSHIP UPDATE
Please complete this Google form to update your local chapter leadership! Then, email your respective regional directors at region#@apamsa.org (insert your region number for #) and membership@apamsa.org.
Don’t know your region #? Check out the APAMSA regional map HERE (scroll to the bottom)!
Have questions? Contact your respective regional director (region#@apamsa.org) and/or membership@apamsa.org.
We are no longer asking local chapters to complete an Excel sheet to update membership. Instead, we will be replacing it with a new membership process.
We highly encourage ALL local chapter officers/members to SIGN UP NOW for our official membership through JoinIt as a paying member! Please join in order to continue receiving exclusive newsletters about national and regional APAMSA events. For more information, including membership benefits and general FAQs, check out our updated website HERE.
To sign up for ONLY general newsletters without membership benefits (non-paying), click HERE.
ABOUT:
APAMSA is a national organization of health professional students and pre-health students committed to addressing the unique health challenges of Asian American, Native Hawaiian, & Pacific Islander (AANHPI) communities. With an organized membership system, we are able to support APAMSA, our chapters, and our mission. All membership fees go back to chapter funding and will support scholarships for the communities we serve.
If you have any questions, please email membership@apamsa.org.
2026-2027 APAMSA National Board Elections Launch
The deadline for interested candidates to apply is Saturday, January 31st, 2026 at 11:59pm PST. Please see below for instructions on how to apply.
1. Join APAMSA: In order to run for a position on National Board, you MUST be an official paying APAMSA member. If you have not yet joined, you can join before applying.
2. Read Instructions: For complete instructions, general rules, FAQ, detailed descriptions of National Board structure, and available positions, please refer to our 2026-27 Election Pamphlet.
3. Join Our Open House: Attend one open house event (for new national board applicants or returning applicants appealing a strike) or an Executive Board (EB) meeting (for new EB applicants). See full details on website.
4. Submit Form: All campaign materials should be uploaded and submitted through our Google Form. Your application will be reviewed by the 2026-27 Elections Committee before it is published.
Questions? Please reach out to elections@apamsa.org.
Response to Mass Shooting at Brown University
On December 13, 2025, a shooting at Brown University claimed the lives of two students and left nine other students injured, with some victims in critical but stable condition. This marks the 75th school shooting incident and the 43rd shooting at a university this year alone. We mourn for the lives lost and extend our support to the victims affected by this tragedy.
National APAMSA strongly denounces all gun violence and remains steadfast in our commitment and desire for comprehensive federal, state, and municipal gun control policies as mentioned in our previous statements and in our policy compendium. We, at APAMSA, recognize gun violence as a preventable health crisis and urge legislators to institute stricter gun control measures.
Measures such as standardizing and closing loopholes in background checks for firearms and increasing funding for mental health programs can be implemented to address root causes of gun violence. Although the 2023 Bipartisan Safer Communities Act has stipulated over $1 billion for improving student mental health, recent administration changes have greatly reduced how that money gets dispersed, denying much-needed mental health professional development grants for colleges and universities. Like disease management, we urge policymakers to focus on evidence-based approaches that have been shown to reduce deaths from gun violence.
In the wake of this recent act of violence, many students may be experiencing fear, grief, numbness, or distress. These reactions are normal, and you do not have to navigate them alone. Support is available both on campus and through culturally affirming, confidential resources listed below.
For Brown University Students:
Brown University Emergency Services
- Mental Health Crisis Stabilization Services: 401-863-3476
- Public Safety Management: 401-863-4111
- Administrator On Call (AOC): 401-863-3322
Brown University Student Services
- Counseling And Psychological Services (CAPS): 401-863-3476
- Free virtual care services for all currently enrolled students
- BWell (Brown Wellness): Online appointment here
- A confidential campus resource for students offering wellness check-ins, trauma-informed support, and help navigating care options after distressing events.
- TimelyCare: More information here
- Brown has partnered with TimelyCare to provide free therapy services to actively enrolled students
- Free access up to 12 teletherapy sessions per year & unlimited access to a library of wellness videos
- Chaplain & Spiritual Support: More information here
- Office of the Chaplains and Religious Life (OCRL) aims to make available pastoral care and advice for students, staff, faculty, and alumni
- Bereavement Group
- When: Mondays @ 7:30PM
- Where: Room 411 of Page-Robinson
- Student Support Services (SSS): More information here
- Contact for either oneself or one’s peers to access collaborative assistance between University staff and the community to provide thoughtful individualized support during complex factors contributing to a student’s distress.
- Contact for either oneself or one’s peers to access collaborative assistance between University staff and the community to provide thoughtful individualized support during complex factors contributing to a student’s distress.
City of Providence Resources
- The Providence Center’s Center for Child and Adolescent Services:
- Open from 8:00AM – 4:30PM (Monday-Friday)
- Family Service RI Crisis Line: 401-854-6678
- Offers counseling and support services for anyone in the community.
- Available for home visits or virtual counseling
- United Way of Rhode Island 2-1-1: Call 2-1-1
- Free and confidential information on mental and physical healthcare, housing, food, and emergency services available in the area
- Open 24/7/365
24/7 Emergency Hotlines
Key reminder: If someone is in immediate danger or talking about harming themselves or others, call 911 or go to the nearest emergency room.
- National Suicide & Crisis Lifeline (U.S.): Call or text 988 for trained crisis counselors
- Disaster Distress Helpline: 1-800-985-5990 or text “TalkWithUs” to 66746
- Immediate emotional support after trauma/violent events
- Asian LifeNet Hotline: 1-877-990-8585
- A free, 24/7 hotline for those in distress. Cantonese, Mandarin, Korean, Japanese, Fujianese offered
- Trevor LifeLine: 1-866-488-7386
- Confidential crisis intervention and suicide prevention aimed for LGBTQ+
Counseling & Support Services
General AANHPI Mental Health Counseling Resources
- Physician Support Line: 1-888-409-0141 (7 days/week, 8am-1am EST)
- Free confidential support for medical students and physicians from 600+ volunteer psychiatrists. No appointment necessary
- Asian Mental Health Collective
- Region-based therapist directory focused on AAPI mental health
- Asians for Mental Health Directory
- Mental health provider directory for AANHPI community (for all 50 states and Washington D.C.)
- National Asian American Pacific Islander Mental Health Association
- Resource list, mental health and behavioral services directory, and blog for AANHPI folks
- South Asian Public Health Association – Mental Health Resources
- Resources for South Asian mental health (organizations, peer support, and provider directories)
AANHPI X LGBTQ+ Mental Health Resources
- The Trevor Project
- Support and crisis services for LGBTQ+ folks in need of mental health support
- Desi LGBTQ+ Helpline for South Asians
- Free and confidential support for South Asian LGBTQ+ individuals
- National Queer Asian Pacific Islander Alliance (NQAPIA) – Healer Network and Therapy Resources List
- API therapists and healers for LGBTQ+ individuals
- National Queer and Trans Therapists of Color Network (NQTTCN)
- Healing justice resources for QTPOC
Self-Care Resources
- SAMHSA – Coping After Traumatic Events
- Evidence-based strategies for emotional regulation after trauma
- NIMH – Taking Care of Your Mental Health After a Traumatic Event
- Self-Care Assessment Worksheet and Plan
For a more extensive list, please visit https://www.apamsa.org/mental-health-initiative/ and look under Mental Health Resources.
Please feel free to reach out to mentalhealth@apamsa.org if you would like to talk and we will work together on how APAMSA can best support you and your chapter.
Authors: David Kim, Mia Park, Brian Leung
Signed: Region I Director, Brian Vu and Warren Alpert Medical School of Brown University APAMSA Chapter Co-Presidents, Jerome Dovan and Sophia Dutton
For questions regarding this statement, please reach out to Brian Leung at rapidresponse@apamsa.org.
For local support, please contact the Region I Directors, Brian Vu and Stephanie Lam, at region1@apamsa.org.
December Ask Me Anything (AMA) with Dr. Steven Chen
Questions? Please reach out to our Professional Development Director, Annie Nguyen, at professionaldev@apamsa.org.

Statement on the Rollback of Universal Hepatitis B Vaccinations
On December 5, 2025, the Center for Disease Control and Prevention’s Advisory Committee on Immunization Practices (ACIP) voted to overturn guidelines for universal hepatitis B virus (HBV) vaccinations at birth despite decades of evidence-based recommendations. Hepatitis B vaccinations are highly successful at reducing the incidence of acute hepatitis B infection by 99% in the United States and preventing progression to chronic HBV infection.
Current guidelines recommend that all infants receive a series of 3 doses of the HBV vaccine, starting immediately after birth and followed by two additional shots at 1 to 2 months and 6 months of age. The newly voted rules will only recommend HBV vaccinations at birth for infants born to mothers with positive or unknown hepatitis B status. Infants born to mothers with negative hepatitis B status will no longer receive a HBV dose at birth. Instead, mothers will need to discuss with their physicians to decide to vaccinate at birth or delay until at least 2 months old. By delaying vaccination by 2 months, this policy creates a window of infection that puts undue risk upon infants of mothers with negative hepatitis B status.
What is Hep B?
Hepatitis B virus is a bloodborne pathogen that can be passed down from mother to child. Acute infection can manifest as jaundice and nonspecific symptoms like fever, fatigue, nausea, and vomiting an average of 90 days after exposure. Infected children and adults can also be completely asymptomatic. Two in three individuals living with hepatitis B infection do not know they are infected.
Unvaccinated children can acquire the virus and develop chronic hepatitis B, which has no cure. Children are especially at risk to develop chronic hepatitis B infection:
- 90% of infants when infected at birth
- 50% of children between age 1 to 5
In the United States, Asian American, Native Hawaiian, and Pacific Islander (AANHPI) individuals represent half of all chronic hepatitis B infections in the United States despite making up 7.5% of the U.S. population.
Why is this a concern?
HBV causes permanent damage to the liver over time, causing cirrhosis and liver cancer. In fact, chronic hepatitis B is responsible for more than half of all hepatocellular carcinomas in the world. The risk of developing hepatocellular carcinoma increases with every year of chronic HBV infection.
Call to Action
National APAMSA strongly condemns the ACIP decision to roll back universal hepatitis B vaccination at birth. Institutionalized vaccine hesitancy is a disservice to our communities, especially to Asian American, Native Hawaiian and Pacific Islander communities who face a disproportionate burden of chronic hepatitis B infections. These rules will undoubtedly reverse the decades-long progress in reducing hepatitis B in the United States and hurt all communities that we, as future physicians, swear to serve. As mentioned in our policy compendium and Hepatitis Initiative, APAMSA is committed to advocating for universal hepatitis B vaccinations and increased funding and awareness for hepatitis screening. We urge that ACIP and policymakers reconsider their decision to pivot from evidence-based recommendations that can potentially harm the next generation of Americans.
Our Current Work
- National Hepatitis B Pledge: Inspired by Stanford’s Asian Liver Center and San Francisco’s Hep B Free, we hope to encourage all medical students to develop habits of screening and advocacy for hepatitis that will follow them in their careers as physicians.
- 2025 Advocacy Day and Hepatitis, Equity, Advocacy, and Leadership (HEAL) Summit – APAMSA hosted the inaugural Advocacy Day on Capitol Hill and the HEAL Summit (formerly known as Hepatitis Conference) in Washington, D.C. During this two-day event, students sat down with Congressional members to advocate for increased awareness and funding for Hepatitis B and heard from the nation’s leading experts on hepatitis and advocacy.
- Grants for Hepatitis Screening: – Apply today to receive up to $1500 for hepatitis screening and education events – applications accepted on a rolling basis.
- Curated list of resources for hepatitis education and screening tools
For questions about this statement, please reach out to Brian Leung at rapidresponse@apamsa.org. For local support, please contact your regional director.

2026 APAMSA National Conference
On behalf of the University of California, San Francisco (UCSF) School of Medicine, we are happy to welcome you to UCSF and San Francisco for ✨ National APAMSA’s 32nd Annual National Conference ✨ from February 20-22, 2026! 🌉
Our conference theme this year is “Bridging Voices, Building Power: AANHPI Solidarity in Medicine.” This year’s conference will bridge academic and community boundaries to identify work being done on the front lines to serve marginalized communities, preparing future AANHPI physicians to serve their home communities through careers in medicine that address health both in the clinic and beyond.
Register for the 2026 APAMSA National Conference here.
We are also currently accepting abstract submissions for the Research Poster Session. The deadline for abstract submissions is January 4, 2026 at 11:59 pm ET.
Questions? Please reach out to conference@apamsa.org.