Statement on the Laguna Woods and Buffalo Shootings
In the latest of a harrowing string of attacks, a Taiwanese church in Laguna Woods, California fell victim to a shooting on May 15th, 2022. Just the day before, Buffalo, New York suffered its own tragedy as a man shot and killed ten Black Americans at a grocery store, in what is currently being investigated as a hate crime. A few days prior to that, a shooting in the Koreatown of Dallas, Texas left three women wounded and is also being investigated as a hate crime.
We lament the fact that these horrifying events are but the latest of a recent string of violent acts, both against Asian Americans and otherwise. It is with heavy hearts that we find ourselves restating our opposition to gun violence so frequently. Yet we also take this opportunity to honor Dr. John Cheng, the 52-year-old AANHPI physician who had charged at the Laguna Woods shooter and, by his sacrifice, ensured that no one else died that day. He has demonstrated immense heroism and selflessness not only in the face of this crisis, but also throughout his faithful service to his community as a sports medicine doctor. We grieve for his wife and two children, just as we grieve for all of the families who lost loved ones over the preceding weeks.
Once more, National APAMSA offers its support to the local chapters and members of New York, California, and Texas during these frightening times, and we encourage you to reach out with any specific ways we can be of service.
For questions or concerns about this statement, please reach out to Eric rapidresponse@apamsa.org
If you are interested in exploring additional ways APAMSA can lend our support during these trying times, please reach out to Nathan at mentalhealth@apamsa.org, or our relevant Regional Directors at region2@apamsa.org (New York), region7@apamsa.org (California), and region9@apamsa.org (Texas).
Statement on the Historic Confirmation of Judge Ketanji Brown Jackson
On April 7th, 2022, Judge Ketanji Brown Jackson was confirmed to the US Supreme Court as the first Black woman, the second woman of color, and the third Black Justice in its 232-year history. APAMSA celebrates this monumental moment as the next step in building an increasingly inclusive society with greater representation of people of color in positions of power.
Supreme Court Justice Jackson is one of many stepping stones for all minority communities. This is especially true when the issues important to communities of color, including that of AANHPI communities, are being decided. In particular, we renew our call for increased representation in the positions of prominence within medicine and academia. The diversity of our doctors must continue to grow for the sake of our minority communities, and our leadership is even more wanting for proper representation. We find hope in the current progress and are eager to see the path continue toward a more inclusive, just, and equitable society.
For questions or concerns about this statement, please reach out to Eric rapidresponse@apamsa.org
Statement on the Brooklyn Shooting
On the morning of April 12th, 2022, a man opened fire on the passengers of a subway train in Brooklyn, New York and ultimately injured 17 people before fleeing the scene. We at APAMSA grieve for the victims and acknowledge the fear that now strikes many New Yorkers’ hearts. We continue to denounce gun violence and reaffirm our support for comprehensive gun reform that would promote the health and safety of our communities. National APAMSA offers its support to all local chapters and its members during these frightening times, and we encourage you to reach out with any specific ways we can be of service.
For questions or concerns about this statement, please reach out to Eric rapidresponse@apamsa.org
If you are interested in exploring additional ways APAMSA can lend our support during these trying times, please reach out to Nathan at mentalhealth@apamsa.org, or the Region 2 Directors at region2@apamsa.org
ACA & AANHPI Health with Dr. Howard Koh
Did you know? The Affordable Care Act (ACA) halved the AANHPI uninsured rate.
Why do I need to care today? 3 million Americans will lose coverage at the end of 2022 if expanded subsidies expire.
How do I learn more? Come to our Zoom webinar with Dr. Howard Koh, former Assistant Secretary of Health in the Obama administration, this Wednesday at 1:30pm ET/10:30am PT. Registration here: https://harvard.zoom.us/webinar/register/WN_sPqUQkSuSRaZexrysZWdNQ
The ACA was signed into law in 2010. Dr. Koh will talk about some of the major benefits the law has brought in reducing the uninsured rate for AANHPI communities. Still, 30 million Americans remain uninsured today. The American Rescue Plan Act (ARPA) passed in 2021 expanded subsidies to help patients buy health insurance on the ACA exchange. But, this critical support is due to expire at the end of 2022 unless Congress takes action. APAMSA will focus this webinar on understanding why the ACA is so important for our community and why we should be activated to fight for public policy that brings us closer to (and not further away from) universal healthcare coverage.
ACA 12 Years Later: Impact on AANHPI Communities
Twelve years ago on March 23, 2010, the Patient Protection and Affordable Care Act (ACA) was signed into law by President Barack Obama. The expansive law included provisions such as an expansion of Medicaid eligibility and the introduction of a health insurance marketplace with federal subsidies to help low-income Americans afford health insurance. Since then, the uninsured rate among non-elderly adults has fallen nearly 40% from 17.8% in 2010 to 10.9% in 2019 according to analyses by the Kaiser Family Foundation.
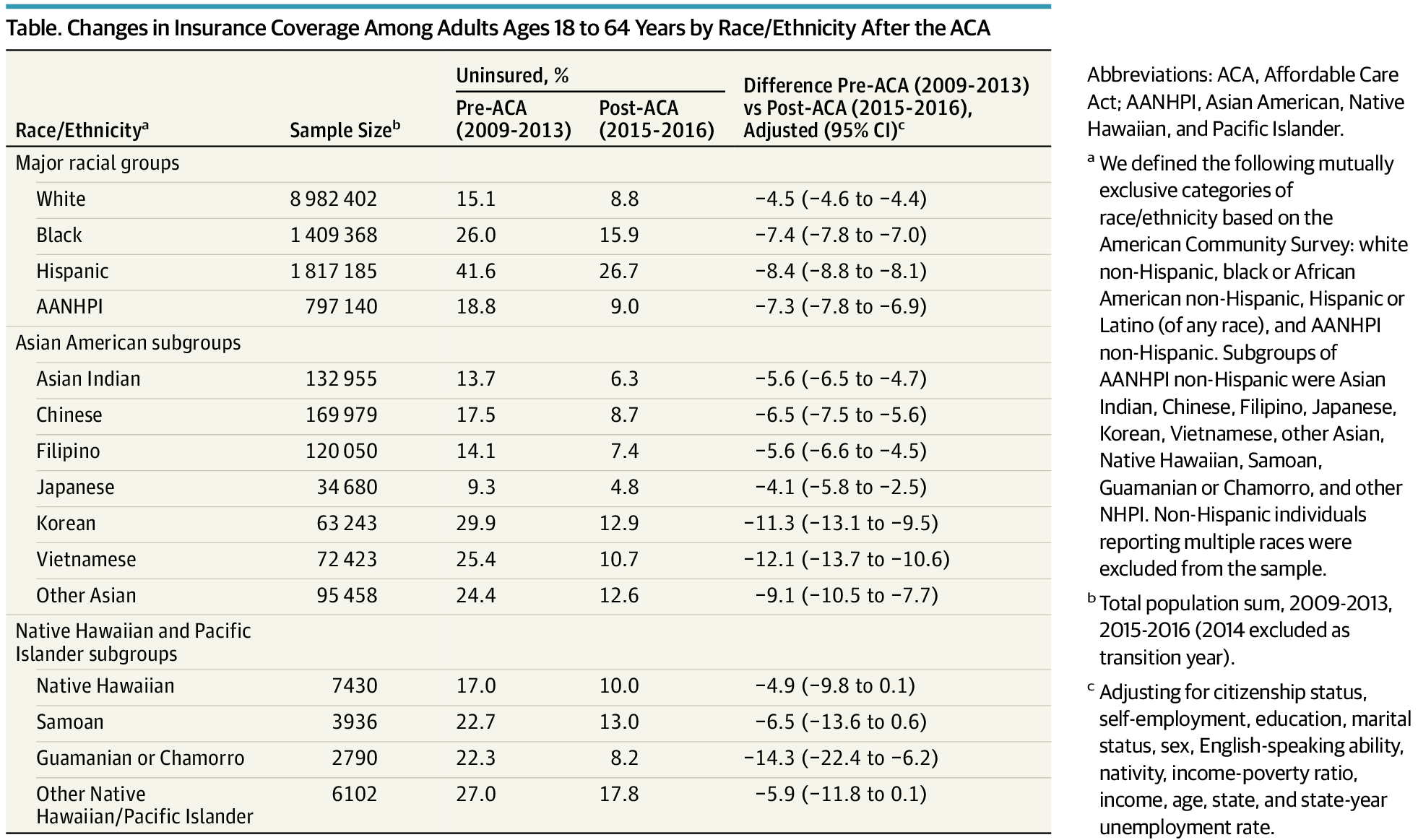
During this weeklong celebration of the ACA hosted by The White House and the Department of Health and Human Services, APAMSA highlights the impact of the ACA on the AANHPI communities. In a 2018 publication by John J. Park et al. in JAMA Internal Medicine, the authors found that the AANHPI uninsured rate fell by more than one half from 18.8% before the ACA to 9.0% by 2015-2016. In particular, the study examined differences by AANHPI subgroup. Korean Americans, who had the highest pre-ACA uninsured rate at 29.9%, saw their uninsured rate fall an adjusted 11.3 percentage points. Guamanian or Chamorro Americans saw a 14.3 percentage point adjusted reduction in their uninsured rate. In context, the ACA nearly eliminated the coverage gap between white and ANHPI Americans. Still, 7.4% of AANHPIs remained uninsured as of 2019 with uninsured rates for other race and ethnic groups as high as 20% for Hispanic Americans. Thus, the ACA may have significantly reduced the coverage gap, but it is clear that substantial work remains to achieve universal equitable health coverage for AANHPI communities and all Americans — a goal APAMSA remains steadfastly committed to realizing in our advocacy.

Dr. Kimara Gustafson
Dr. Kimara Gustafson
Assistant Professor @ UMN
Key Words: adoption medicine, transracial families, cultural identity development, research, academia
Welcome everyone to the APAMSA AANHPI Health Issues Interview series, where we’ll be interviewing researchers, policymakers, community-based organizations, and other experts on health-related topics that affect the NHAAPI community. My name is Grant Wen and I’m the health advocacy director at APAMSA National. For this interview, I would like to welcome Dr. Kimara Gustafson. Dr. Gustafson works as a pediatrician at the University of Minnesota focusing on adoption medicine and has done research on children with special health care needs as well as racial and cultural identity development for children of transracially composed families.
I’m a practicing pediatrician up here in Minnesota, in the Twin Cities, specifically in Minneapolis, and I did medical school and residency here as well. I originally grew up in upstate New York, just north of Albany and then came out here for school. I have extended family in the area, so I have a little bit of a connection, but mostly came for school. I kind of always knew I wanted to do pediatrics. I was playing around with family practice or not, but ultimately kept coming back to pediatrics. But then within that, I really lucked out in that the University of Minnesota is unique. We have an adoption medicine clinic, there’s just a handful in the country, and this is definitely the one of the oldest and maybe most comprehensive, so I was able to do a rotation there, and eventually have been able to stay on as faculty. I practiced for a couple years in the community as a general pediatrician, but came back to be on faculty. And part of the reason that it’s something that I’m interested in is I have a personal connection. I was born in Korea, and then adopted as a young infant, when I was about seven months old. My parents are American, my mom is white, of Lutheran background from Minnesota. And then my dad is Jewish, and he grew up in Long Island in New York. So kind of a lot of different cultural aspects that have kind of come together as I was growing up, but it kind of makes up our family.
The clinic is over 30 years old. Originally, it was founded by my mentor, Dr. Dana Johnson, and essentially was founded out of necessity. He is a neonatologist by training, and when he was starting to kind of put together his family, he adopted a son from India. And at the time, his son was quite young and had a lot of issues that we think are common to lower resource areas, such as malnutrition, a lot of infectious diseases, and parasites. And then had kind of sequelae from that in terms of delayed development and growth. Being the wise clinician he was, he looked around to see who he could go to in order to navigate this for his son, but he realized that didn’t really exist.
So he put it together and essentially formed his own clinic. Historically, the clinic has been more geared towards international adoptees. What’s kind of nice and unique about the clinic is that we’ve been able to follow the trends of adoption, which vary based on state department and geopolitical events. So there are trends in international adoption. The last 15 years the trend has been just overall there’s less international adoptees, so our clinic has started to kind of pivot a little bit. We still see children that are internationally adopted at various stages in their adoption, but now we’ve really expanded on the domestic and foster care side. I would say on any given day, I would do probably 70%, maybe even 80%, domestic and foster care medicine, and then 20 to 30% what people think of stereotypically with adoption (international).
We used to think adoption was more of a static event. If you were adopted, with nature versus nurture, nurture would take over. If you had the right environment, then any potential risk factors that you experienced early in life would be overcome, or potentially overcome.
Now research has evolved, especially piggybacking on the work of Felitti and his group in California with the adverse childhood experience (ACE) study. We know that ACEs, even if the ACE is theoretically buffered by the fact that they were adopted into a middle class family with resources, put individuals at higher risk for health issues like heart attacks, cardiovascular disease, hypertension, diabetes. Similar to that, we know that ACEs may need to be proactively addressed and more proactively buffered than what we previously thought or had hoped. In foster care, international and domestic adoption, if at any point a child has a caregiver transition, then there are long lasting health effects, even if a child is adopted domestically at birth. We used to think if the adoptive family comes to the hospital and takes a child home, they’re a blank slate, but now we know there’s so much influence from the prenatal environment. And so anytime you have a caregiver transition, that potentially can influence or have implications in that person’s ongoing health. What I’m interested in is the next step. We know that ACEs are a thing, but how do we buffer? It’s not, it’s not really fair or helpful to someone to give them just an ACE score. Ideally, we would give an ACE score and then try to help mitigate that. Does it mean that you need additional screenings? Does it mean that you need additional support in terms of how to buffer stress, because maybe your body doesn’t handle stress as well as your peers?
Specifically for the kids that I work with, by and large, they are transracially placed. Not to get too much into the geopolitical side of it, but both internationally and domestically, the families that children are being placed with usually have better financial resources. It’s very expensive to adopt, and it’s still expensive to adopt through the foster care system or domestic adoption, and so the current predominant adoptive family consists of middle class white parents, and the children that are in the system to be adopted are usually brown, black or NHAAPI children. There are kin adoptions, and then on the domestic side, so you’re being adopted within the family, but even with kin options, it’s not necessarily that they are going to be the same race or culture. Often we’ll see a kin adoption where maybe the adoptive family still identifies as white, but the child is mixed race, but gets adopted to the white side of the family. But they’re the only black or brown kid in the family.
What I’m interested in is what we’re learning about racial trauma. Do we think of racism as an ACE? My research question is—-for parents who are not same-race matched, do they have the tools and information that would best set everyone up to try to buffer that racism? Historically they haven’t. So how do we help them to improve on that? Historically, you hear anecdotally, within the adoption community, that parents have said, “Well, I don’t think of you as being different. I just think of you as my kids.” The origin of that is very admirable, but it usually results in the kid feeling canceled or minimized to some degree, because they’re thinking, “Why am I having these racial racist experiences that my parents don’t believe are happening?”. Or they just say that the kid is making too big of a deal about it and that they shouldn’t let it bother them. The other thing is that sometimes, unfortunately, it’s coming from within the family, either the immediate family or extended family.
I would say that parents don’t have intent to cause harm to their child, but they just might not have the knowledge and the tools to really help to address it. And in general, with everything, if we’re uncomfortable about something, we kind of just try to avoid it. We’ve come a long way in the adoption world, but there are still questions about many things. For domestic adoption, let’s say, I still get questions where parents are like, when do we tell them that they’re adopted? And from my standpoint, I say as early as possible, but some families feel that they don’t know how to have this conversation. So the default is they don’t, and then it gets to be kind of this elephant in the room, like, now they’re 8 or 10 or 12. And they don’t know how to really explain it. Whereas we know by research that if you had those conversations from a younger age, it wouldn’t have potentially become such a big thing.
I think it’s been great because there’s been a lot more resources out there on how kids perceive race and at what age do we start talking about it. We know by research that kids as young as six months old will perceive physical differences. They show a preference for a caregiver who looks like their primary caregiver. So, if you have a translationally composed family, and the infant is black or Latinx, then the infant will develop a preference for other white adults. We also know that if you go up developmentally, children of color often will start to have a social preference for the dominant or the majority color when they get to interact in a mixed group.
It’s not uncommon that children in that kindergarten or preschool will say, “I wish I had blonde hair, I wish I had light skin.” If you have a family that’s the same race, then when the kid goes home,theoretically, the parents would say, “Oh, no, you’re beautiful the way you are. You look just like dad and mom.” So they have that representation and buffer within the home. So then the question is, what do you have when you have a transracial family, and you don’t have that kind of reflection in your home or in your family?
So if you’re in school, and you’re five or six, and you say, “Oh, I wish I looked like Elsa,” you go home, and everyone in your house looks like Elsa, except for you. Then it starts to impact your self esteem. In adolescence, you’re developmentally supposed to be kind of figuring out who you are and how you fit in your environment. For kids who are adopted or in foster care, a lot of those questions are often answered either because they reconcile with those around them, or it’s in opposition. Everyone’s different, but that time can be really stressful, in the sense that they start to really think about where they come from, and if they’re, like, “I don’t know where I came from.” Oftentimes this has to deal with the narrative around the first or origin family, what some people will call birth families. The adoptive parents, not with the intent to be harmful, will often say, “Oh, your birth mom couldn’t keep you because she was too young, or because she had health issues, substance use.” It’s not uncommon that I’ll have teens who start to think “Oh, is something going to happen to me?”—-because they get so much information from the community or the media and school about genetics and things that are inherited. I actually had one teen who said she was worried she was going to get pregnant, although she’s not sexually active. She was really worried she was gonna get pregnant because that’s what happened to her mom.
The other thing I see is that racial or cultural identity gets put on the back burner, because they’re just dealing with all this other stuff. And then it’s not uncommon that they get to college, and all of a sudden they get to meet other people of their race, particularly if they’re coming from a homogenous community. Unfortunately, they often end up getting rejected from that community too, because they’re like, “you’re not a real Asian, or you’ve never used chopsticks before.” They get stuck in this kind of catch 22 and feel rejected by both. And keep in mind this is all happening in the midst of the larger issues of identity. We know that mental health issues are more prevalent within adoptees, and if these things are left unaddressed or undersupported, they will impact self concept, self esteem, and contribute to depression and anxiety.
I’m actually in the process of trying to create formalized anticipatory guidance for promoting racial and cultural identity. Historically, we’ve thought of that as something that happens in the home. But again, like, what happens if your home doesn’t match? Most parents want to support their kids, but in the absence of knowing how to, they might not.
Going back to the research, if we know that kids are starting to identify different races and cultures as early as infancy, then similar to anticipatory guidance, where you talk about vaccines, water safety, wearing seatbelts, you try to have the conversation to tell parents that their kids are recognizing that they look different than their siblings or their peers. This involves helping the parents have a developmentally appropriate conversation and making sure that they have materials that are able to best represent the child’s needs.
The hope would be that if the child feels like this is something that their parents want to support, then they feel empowered to self identify. When they get to adolescence, they’ll be able to maybe make connections, so that this process doesn’t get deferred until the young adult stage. For teenagers, even if you’re not adopted or translationally placed, junior high is kind of that time where you’re like, “Okay, who’s where, who’s my group.” I feel like for these kids, they often just stay with the group of their parents instead of finding their own group, and then what happens is when they get to college, it gets turned on its side. This exploration doesn’t have to replace or supersede their family culture, but can kind of intersect a bit better. Research shows that when kids are younger, they are buffered usually by their parents when they experience stress, but when they get older into adolescence, the buffer for stress is usually their peers. So we hope that we’re able to give them the tools to find that friend group that they really feel can buffer. For instance, if they experience some sort of racism, then maybe they have enough peers who are like, “yeah, that sucks,” or “this is what I do when that happens,” instead of if their peers are all the same group as their family and these problems get dismissed. Or perhaps the racism coming from that peer group itself.
I have personal experience with this, but I think this last year has been really interesting in that there’s been a lot of discussions within the adult NHAAPI adoptee group of where we fit in. I was actually talking to Dr. Jonathan Tolentino, a med-peds doctor in Miami, about this concept that within the black community, parents will have the talk with their kids about ,”here’s how society is going to view you, they’re going to view you as an angry black kid.” I don’t have direct experience, but just from talking to friends, and that it’s not as common that Asian parents will have that talk with their kids. And if anything, they try to kind of do as much as they can to kind of buy into that kind of concept of assimilation. Like, yes, we are going to be the model minority. Yes, we are always going to excel, and through our kind of success, you’ll see that we are worthy of acceptance.
This last year, the young NHAAPI generation is like, “you know what, if we strive to fit ourselves into the model minority myth, and we’re still going to experience racism and discrimination, why should we try to fit ourselves into that?” Because it’s obviously not working. Within the NHAAPI adult adoptee community, now, is this question about where we fit in. Because, historically, the media has tried to pit everyone against each other. The adult adoptees feel like, “well, we look Asian, but we were raised culturally white, so we have some privilege that even Asian Americans might not have due to the proximity to our parents and the white community. And we can serve as a bridge.”
There’s also been discussions where, and this is a gross generalization, but historically in certain Asian countries, there is a preference for lighter skin, and that prejudice is maybe more present in the parental generation. What’s interesting in the adult adoptee community is that there are some parents who are very comfortable in terms of issues about race and racism. Sp for many adoptees, they can say that they lived in a very diverse community, and at least from the home, they didn’t get some of that kind of teaching that maybe had racist overtones. So I think it’s an interesting place to be, because I’ve seen a lot of mobilization and coming together around these issues and feeling a bit more comfortable to occupy space and try to be advocates in all these different ways.
In general, I think your generation is kind of firing away much farther ahead because I think you’re just like, “we’re tired of having to deal with some of the microaggressions or things that are considered micro but don’t feel micro,” and “we’re tired of having to suck it up and be told that we should just let it roll off our back,” whereas I think the older generations are, like, “don’t rock the boat.” This is also one of the reasons I love working with trainees, because you guys help keep me honest. And also I learn so much from you guys in learning that sometimes you have to upset people to get the change that you want.
I: I wanted to thank you so much for taking time out of your schedule to share with us. This has been a super enlightening talk. I knew next to nothing, essentially, about adoption medicine. But I think I’ve learned so much through this conversation, and I hope that our listeners will as well.
G: Thank you so much for having me and just let everyone know if anyone has questions for me. I’m always available, you can email me. Thank you so much for this opportunity.

Dr. Lin Fan Wang
Dr. Lin Fan Wang
Former CMO @ FOLX Health
Key Words: LGBTQIA+ community, critical race theory, reproductive health and justice, transgender care
I: Welcome everyone to the APAMSA NHAAPI Health Issues Interview series, where we’ll be interviewing researchers, policymakers, community-based organizations, and other experts on health-related topics that affect the NHAAPI community. My name is Grant Wen and I’m the health advocacy director at APAMSA National.
For this interview, I have the pleasure of introducing Dr. Lin Fan Wang. Dr. Wang is a family medicine doctor and the Chief Medical Officer at FOLX Health, a queer and trans telemedicine company. In addition to her clinical work, Dr. Wang is a cofounder of Centering Equity, Race, and Cultural Literacy in Family Planning (CERCL-FP), whose mission is to use critical race theory and reproductive justice frameworks to dismantle structural racism within reproductive health care. She created and moderates the Gender Affirming Health Care Listserv, is on the board of Medical Students for Choice (MSFC), and is a fellow at Physicians for Reproductive Health (PRH).
Sure, absolutely. In academics, we often start off with where we went to for education, but I’m going to start off with my immigration story, because I feel like that’s so relevant to NHAAPI communities. So I was born in Taiwan, and then I moved to the US when I was around four or five years old. I grew up in the white suburbs of Michigan and I was really rebelling against medicine–I didn’t want to do it. I think just because in NHAAPI communities, it’s like you have three options for jobs—-you go into medicine, you become a lawyer, or you go into engineering. So I was like, I’m gonna rebel against that. But then I was doing some work in research, clinical research, and I found that it was just really interesting to me. Not so much the research part, but the clinical and the medical parts. And so that’s kind of how I got into medicine, and I ended up going to medical school at the Albert Einstein College of Medicine in the Bronx, New York.
And at that time, I was thinking maybe pediatrics because I liked kids, maybe psychiatry, because I was interested in people’s minds and how they make decisions. And as I was going through my clinical rotations, I realized that I liked all of them, with the exception of surgery. I felt like in surgery, my hands were always in the wrong places. Even though I held them where the surgeons told me to hold them, they were still the wrong places. So I thought that surgery was not for me, I can’t, I don’t even know where to put my hands.
But because I liked doing everything, I decided to go into family medicine. And as part of my family medicine work, you know, I just loved it. It really drew me in because one, I was able to see people of all ages. But I think the other was just the culture of Family Medicine is around taking care of entire families, and also really thinking about how the community piece affects individual health. And then as I was getting into family medicine, it was also about full spectrum care. It was about prenatal care, seeing kids, and the elderly. And as part of that, I realized, you know, as a person is coming to me, I should be able to take care of whatever issues they’re having. So that includes like mental health and includes pregnancy and abortion care. And it should include LGBT care as well.
And so after I finished finishing residency, I was really thinking about, what do I do now? Right? And I did end up deciding to do a fellowship because I felt like you know, I wanted a little bit more time to explore what parts of medicine I actually like. I wanted some more training specifically around how to train other people and provide health care. So I did end up doing a family planning fellowship. But of course, for all of you students out there, you don’t have to do a fellowship, it’s perfectly fine for you to finish your residency and then just go directly into practice.
But I did do a fellowship and then afterwards, I was kind of also trying to decide what I wanted to do. And I found that advocacy was just immensely important for physicians to be a part of. Advocacy is really scary, right? I think especially for NHAAPI folks, because we’re kind of taught to be quiet, to not make a lot of waves, to kind of just focus on your job. But advocacy is hugely important. Legislators really listen to physicians when they speak out, and especially when they’re passionate, and they’re speaking out on behalf of their patients. So I did end up doing an advocacy fellowship. And then after that, I was like, “Oh, so I can’t keep going, I can’t keep training, I actually need a job now.” But I was thinking, “Well, what do I actually want to do?” And that’s how I came into really focusing on care for the LGBT community, I was looking for a job that was outside of New York. So I came to Philly, and I worked at Mazzoni Center for a while. And it was just really a wonderful match in terms of my interests, my own background. I think for me, I really enjoyed working with my community, the queer community, and in particular, the clinic had Title V funding, and we also had Ryan White funding to be able to do HIV care. As a part of that we’re also providing a lot of care for marginalized communities, including NHAAPI folks.
I’m happy to share more about how I came into FOLX health and why I decided to do telemedicine, but I also work with CERCL FP (Centuring Equity, Race and Cultural Literacy in Family Planning). As part of that work, we are a group of former family planning fellows who are all either people of color or co-conspirators, who are creating a training curriculum for clinicians and family planning, who are wanting to incorporate reproductive justice and critical race theory into their work. I am also working with another group of family physicians of color in abortion care, and we are working on a separate project thinking about how we can best support physicians of color who are interested in providing reproductive health.
In terms of FOLX health, I think it was a combination of things when I was working at Mazzoni Center. If you’re not familiar with Mazzoni Center, it is a clinic specifically for LGBTQIA populations, and during my work there, we realized that patients were traveling for hours to get to us. Care for LGBTQ communities should be part of all the work that we do, right? So no matter what specialty you’re in, you should be able to take care of a patient who identifies as queer or trans, but I was finding that patients were traveling specifically to come to our clinic and so I thought well, maybe I should move into the primary care world and think about how do I train other family physicians or their primary care physicians in incorporating this type of care into their practice.
I was doing that for a while when I was working at Einstein hospital, and then COVID hit and we had to provide telemedicine, and I found that it was a completely different experience for my trans patients. Because that meant that they could do our visits in the comfort of their own home. It meant that they didn’t have to worry about being out in public and possibly being misgendered. They didn’t have to worry about “what do I wear when I walk into the hospital?” or “How do I present myself?” “Is someone going to make comments about how I look?”. All of that went away and I was able to see them in a place where they felt safe and comfortable. Part of that was just really improved access right? My no show rates really went down. And they were able to actually come and be present during their visits. They were much more relaxed. And so I thought, if I’m really thinking about access, I should really be thinking about telemedicine. And then I found FOLX health. They were a new startup looking for clinicians to work for them. And I was like, this is a perfect match of all my interests and joined.
So I think one example of critical race theory ties into healthcare is about counter narratives. We work within these dominant narratives, where it’s really about a world where everyone is white, straight, cisgender. Christian, and if you’re not part of that dominant group, then there are stories being told about you and your community, and you have no part in that. So these are stories like, “all trans people have hard and difficult lives,” or “queer NHAAPI people don’t exist.” A lot of it is thinking about who gets to tell the stories and how the stories are told. And from the counter narratives and thinking about dominant narratives, the way that I started to think about stories with my patients, is “how do I create a space in which they tell the story of themselves however they want to?”. So it might mean that they don’t even tell their story, right? If they’re like, I don’t trust you enough, or this space doesn’t feel safe enough for me to share my story. And then for me to be okay with that. Or for them to say, “you have to know all of my life in order for you to even take care of me.”. So then we spend 15-30 minutes just talking about their life story. But it’s really about creating the space in which they own and have the power in deciding what is told. I think the other piece is just really being intentional about, when I ask questions, how I ask them. Do I think about autonomous decision making in everything that I ask? And I think particularly for NHAAPI and queer communities, there’s a lot of questions that can be very invasive, or feel very invasive. Things like sexual health history or decisions about end of life, cancer diagnoses. So it’s a lot about letting me understand where you are and letting me tell you why I’m asking you all these questions, and then you can decide how you want to engage in that. And they might say, “No, I don’t want to talk about my sexual health,” and for me to be okay with that.
I find that FOLX health allows me the opportunity to really tailor things. And so part of our process is because we know how damaging the healthcare system can be and that many queer and transgender (particularly transgender) patients have experienced harm, either verbal or physical in the health care setting. We know that they bring all those things with them to the visit. So part of the process is to allow patients to decide, do they even want to interact with the clinician at all. So they could elect to just not even have a visit with us, but they would fill out a questionnaire and they could answer questions that we think are clinically relevant. So we give them power to not have a visit with us. But when they do decide to have a visit with us, I usually end up starting out being very open ended, just being like, this is your time. We have 15 minutes, 30 minutes, however long it is. And would I say that “you decide what happens during this visit. I want to make sure that we answer all your questions, and you can share as much or as little as you want.” And then that kind of sets the tone for that for that visit.
A lot of it is all around thinking about culturally relevant care, especially being able to provide care that is not just culturally relevant, but specific to that individual person. Because the queer and trans community, the NHAAPI community, we’re all extremely diverse. And we all have our individual specific needs. But I think it’s like, in particular for the queer and trans community, is thinking about how do we make the environment gender neutral, and not make assumptions about people. And that’s true for the NHAAPI community as well. Let’s not make assumptions about what someone thinks or what their values are just because they are NHAAPI, right? Because you have NHAAPI folks who grew up in the US or who have had several generations in the US, right? And that person’s gonna be different from someone who just came to the US as an adult. Or if they came to the US and have gone to graduate school versus someone who has a second grade education, right? Those are two very different people with very different needs. It’s all about one, trying to make the environment gender neutral and affirming as possible, but the other is really not making assumptions about people, but asking them questions.
I think another big issue for the NHAAPI community is translation services. I think that in terms of the NHAAPI community, you’ll find that communities immigrate either regionally or by country, so they kind of tried to gravitate towards each other. And so part of it is making sure that whatever service you’re offering is relevant to the communities that you’re serving.
I think it’s scary and hard because, as a physician and someone who works in trans health, I know that access to trans health care for children and for young adults is extremely important for their success. You had brought up health disparities before among the LGBTQ community, and part of what causes health disparities is not having support. And support can look many different ways. I think when people think of trans health, they think things like medication, hormones, and surgery.
But that’s not the case for many trans people, and especially not for trans and gender diverse youth and children. It’s really about—- are they or their families getting the right information? Are they being supported and whatever their gender journey is? We know that when kids are supported in their gender, they thrive, they do well, when children are not, that’s when it causes all these horrible health disparities. The other thing to know is that there is a lot of evidence based research around what helps keep these children safe. And these legislations are all the complete opposite of that. They are really about transphobia, hatred, whereas it should really be about the families and children making the decisions that are right for them with their health care provider.
In terms of what we can do, it is mobilizing your state. If you have the opportunity to speak out against legislation, call your legislator. I know, it’s really scary, so if you can, do it with your friends, get a group together, or just make a script. They really just want to hear from you. And you just speaking out can make such a huge difference.
I: Thank you so much for sharing. That’s something that we’re definitely trying to do at APAMSA, giving students the resources to know how to advocate for their communities. And that’s definitely something that we are interested in continuing to do in the future as well. Thank you so much, Dr. Wang, again, for taking time out of your schedule to do this interview.
Siya Qi
Siya Qi
Senior Program Manager @ Asian Health Coalition
Key words: Community based organization, AANHPI representation in research, community engagement
I: Welcome everyone to the APAMSA AANHPI Health Issues Interview series, where we’ll be interviewing researchers, policymakers, community-based organizations, and other experts on health-related topics that affect the NHAAPI community. My name is Grant Wen and I’m the health advocacy director at APAMSA National. For this interview, I have the pleasure of welcoming Siya Qi. Siya is the Senior Program Manager for the All of Us research program at the Asian Health Coalition (AHC). She works with Asian engagement and recruitment core partners across the nation to engage and educate Asian Americans, Native Hawaiians, and Pacific Islanders on the All of Us research program.
I work at the Asian Health Coalition and also the Center for Asian Health Equity in the Chicago area. I am an immigrant from China and I moved to the States five years ago. And I got into this field because of my grad school research on senior care and senior living. During that process, I interviewed a lot of Asian immigrants, especially elders, and then I found a lot of health equity issues, not only for seniors, but also for young immigrants too. That’s how I got interested in this, and then after graduation, I was really lucky that I found this program and this organization. I applied for the job and luckily got accepted and it’s been one and a half years now.
The project that I’m working on now is called the All of Us research program. It was actually initiated by the National Institute of Health and hopes to invite at least 1 million individuals living in the US to help build one of the most diverse health databases in history. This program aims to provide diverse databases to researchers with diverse backgrounds, and hopefully, the researchers can use the data in the database to make discoveries to find patterns and discoveries on things like cures to certain diseases like cancer and dementia. By including underrepresented communities, they hope to better address health disparities for future generations especially. So that’s what I’m currently doing.
We are involved in this program as one of the National community engagement partners. We’re working with our 15 partners across the country to engage and educate Asian Americans, Native Hawaiians, and Pacific Islanders. NHAAPI communities have continued to be underrepresented in research, which has really caused a lot of problems. I’m not sure you guys do, but I know friends who take medicine from our home country, just because some medications don’t work for us in the States. And normally, we think that’s normal. And we never think about how we can better address it or how we can solve it and why it’s causing it. It’s really because we are underrepresented. We’re not involved in these types of research. I think the All of Us research program is a really good opportunity for us to gain representation, to be seen, to be heard. And then for the future generations, hopefully our kids or grandkids won’t need to travel back to another country to truly find the medicine that really works for them. That’s the hope, so we’re working with the community to really spread the word and promote this program.
As for the Asian Health Coalition, it is a community based organization located in Chicago. We do have cancer prevention (colorectal cancer screening), Hepatitis B, and a million other programs. We normally do a lot of health education, health literacy, and health promotion in local communities, especially for underrepresented and underserved communities locally in Chicago or Illinois. Not only do we focus on the NHAAPI communities, we also do work with African American, Hispanic, and other communities historically underrepresented and underserved, providing them with health resources and education.
There have definitely been new challenges after COVID. In the past, community work was 90% in-person events, like gatherings at community centers where individuals could share food or celebrate festivals and special holidays together. But due to COVID, people couldn’t gather and don’t feel comfortable doing so. So that was a huge challenge, especially for some of our community members, as the majority of clients we serve are the elderly with limited English proficiency, and really limited knowledge and even access to internet and digital devices.
COVID really changed everything for our organization also. First, we couldn’t work in our office building, so we had to work from home.Second of all, we had to transition events and projects to digital platforms, and to do so, the initial steps we took were to do digital literacy programs for the seniors in the communities that we serve. I know that some of our partners called the seniors individually and gave them instructions on how to use Zoom, how to create an account, etc. And then they went into health education and even social gathering through zoom and other digital platforms. So that was really new to us. But surprisingly, they all adapted to the digital world fairly quickly. The seniors seemed to become very familiar with the platform, and they really enjoyed talking to each other. So that’s really going smoothly for now, but with things slowly transitioning back to reopening, I’m sure there’s going to be new challenges, and we will see how we can adapt to any new situations.
We also have been supporting local businesses since the pandemic. For example, we ordered 1000s of masks from a local Vietnamese shop. That’s one of the ways that we’re supporting the local community. We also collaborated with the local businesses in Chicago, where they helped us distribute the resources that we created, such as handouts with in-language materials and resources for local communities.
Right after the pandemic hit, everyone—-but especially the communities we serve (elders with limited English proficiency)—- had been isolated at home. So we collaborated with APAMSA to create a student ambassador program for students to call seniors who felt isolated to make sure they felt supported enough to meet their physical and mental needs. Especially after the anti-Asian violence, there was a huge increase in mental health needs for the coming from the elders in our communities along with even more hesitancy in going out. We’ve received some good feedback, especially with the program that we’re doing with APAMSA. Seniors across the country appreciated the company and the conversations they had and also the students helping them process COVID information and also the vaccine.
As an organization we responded and had events and ongoing protests, like many other groups across the country. There were also digital platforms where people could sit together to share and process as a group to think about how to move forward. We also did an Asian Profile Series on social media to introduce the diverse culture and uniqueness that each subgroup within the Asian community has. On social media, we also shared some of the great work our partners have been doing. One thing that we don’t want is to really focus on the bad side of things. We want to really create a positive environment, and for everyone to take a minute to appreciate culture and diversity rather than dividing one group from the rest.
In particular, Chinatowns across the country were severely impacted, because you see these videos of seniors getting hurt on the streets, and you feel this sense of danger when you walk on the streets. Even for myself, being an Asian female, I had this sense of vulnerability walking in the streets even before the pandemic. And then after all of this violence, I felt even more insecure in open spaces, and I think that was really common for residents in Chicago. In Chicago locally, we had a lot of protests against AAPI violence. We appreciated all the people who traveled across the country to support this initiative. In the past, Asian communities tended to be quiet, because we did things within our communities, we solved our own problems, we weren’t really vocal, but this time, we really stood together to fight against these crimes as a whole group. That was really inspiring and touching to see. After protests, although things were not back to normal, you feel a bit better. As an organization, we also dedicated one staff meeting to really talk about anti-AAPI violence, in part because unfortunately some of our colleagues had experienced some of that. We also ordered T-shirts with “Stop Asian hate” from a student group in Chicago, so that was one of the many ways that we supported this initiative alongside our local community.
When we were really promoting the “All of Us” research program, we used vaccines as a way to encourage them to join the research program. We said that just because past medications might not have worked, but if NHAAPI individuals are more represented in data, we might be included in future vaccine development initiatives.
When the vaccines actually came out, community members started to ask questions like, “How do you know this vaccine is gonna work for us?” This really required us to put ourselves into the shoes of the committee members. We hadn’t faced such a pandemic and challenge—-for our generation, our mother and father’s generation, or even that for our grandparents.
What our partners ended up doing was a lot of online education on the vaccine—-how it works, how the trials were, how would that impact our Asian communities, and then how the vaccine could help. This was not to push them into getting the vaccine, but just to deliver the information and give them resources to decide on their own. They also were given in-language materials and invited experts to answer questions. I know we have one partner in Boston that serves the elderly population, and they ended up calling every senior resident, telling them about the vaccine and giving them education. Andy from APAMSA actually was part of that conversation, too. He helped explain how the vaccine works, how it would impact your health and that of the community. I think that community ended up having a very high rate of vaccination, so it was a huge success. And we could see those across the country without penalties. From our experience, hesitancy really was a challenge at the beginning. but if you give the community members enough resources and information, they can have their own way of responding and can make their choice.
I think hesitancy really decreased as time went on, but this might be a biased opinion because those who come to our organization are the ones eager to learn more and want resources. The rest of the community members don’t come to us normally, and I can definitely still see some hesitancy there, although I do think it’s getting better gradually. This is partially because with more people getting vaccinated, they can see the reactions and side effects.
I don’t think the government has done great helping communities with limited English proficiency. And this is why the community based organizations are here. I don’t think they don’t want to help, they’re just not equipped with the ability to do that. We know that when communicating with the community members, it’s not only about language, it’s also about cultural things. There are many aspects to take into consideration, from who you speak with, to the channels you’re using. If you’re talking to elders, they probably don’t have social media, so you can’t communicate through Twitter. Using print materials would be much better. It’s also about how you’re presenting this message.Are you using graphs and giving them a research paper? That’s not going to help, and that’s also why we step in as community based organizations. We create materials that are adapted linguistically and culturally for our communities. We have images that really resonate with them, they see similar faces, and we make sure to cover some of the more taboo cultural topics in a way that is digestible.
Honestly speaking, I don’t think the local government did a good job, especially for our community members. This is primarily because they don’t have the flexibility and ability to reach our communities and especially for our native Hawaiian communities, they don’t really trust authority that much, understandably so given their history with the US government. We get that, so we’re taking the information from the government and translating it in ways that the community members are more likely to accept.
One lesson I learned from COVID and from health education and health equity work is the importance of collaboration, such as what we had with APAMSA. For the following months, we’re going to relaunch the student ambassador program, and we’re going to send out another round of applications. This time, we’ll have student ambassadors who are going to do three different things. One may be still involved with wellness, a second role would be doing health education, and the last will be video making and producing. We’re also going to have a separate project that’s focused on student research. We hope to invite several students to join us as student researchers to utilize the “All of Us” database. I think over 300,000 participants’ data is in that database. Please join us, and you can contact me if you’re interested. We really love working with you guys.
I: That sounds like very exciting next steps that you’re taking. And I’m sure that many of the APAMSA members and other medical students will be very interested in all these opportunities.
S:Thank you so much for having me here. It’s always a pleasure to talk to you guys. And look forward to working with you again!

Dr. Nicole Barnes
Dr. Nicole Barnes
Assistant Professor of History @ Duke University
Key words: History of Chinese medicine, History of global health, research, health humanities, academia
I: Welcome everyone to the APAMSA AANHPI Health Issues Interview series, where we’ll be interviewing researchers, policymakers, community-based organizations, and other experts on health-related topics that affect the AANHPI community. My name is Grant Wen and I’m the health advocacy director at APAMSA National.
For our first interview in this series, I would like to welcome our guest Dr. Nicole Barnes. Dr. Barnes is a professor of history at Duke University with co-appointments in the global health department and the program in gender, sexuality, and feminist studies. Dr. Barnes holds a place very near to my heart because she was my thesis advisor back in my undergraduate years, so without further ado, let’s welcome Dr. Barnes.
B: Thank you for that introduction, Grant. So yes, like you said, I’m an assistant professor at Duke. I teach the history of Chinese medicine, history of global health, and general courses in history of China as well as global history of medicine. The history of medicine is my greatest passion, so I’m delighted to bring those insights to bear on the questions of the day.
Yeah, the story really goes back to my childhood. I moved with my family in second grade to Logan, Utah and it was a small town where almost everybody was Mormon but I was not, and so in seeking out the non-Mormon friends, I found the Asian-American community and just from a very early age, became very comfortable with my Asian friends and their grandparents who didn’t speak English and ate different foods. I just kind of fell in love with Asian cultures and gained a sense of comfort in those spaces, something that really helped me later on as a college student, as I pursued deeper interests in foreign languages and cultures. I was actually a French and Spanish major but then I became a dual minor in Chinese language and Asian studies. I spent some time in Guiling, in Guangxi Province in mainland China as well. My Chinese teacher at the time, Chiumi Lei, who is now at Rice University, encouraged me to go into graduate school and wrote stellar letters of recommendations so I got funding, which was really important because I came from a family of low economic means, so that funding to continue my studies was essential for me. That’s something that I try to continue to do as a professor now—-to continue to mentor, sponsor, and assist students to pursue their lifelong passions, even if they don’t have the economic needs to do so personally.
So that’s one aspect. And then the history of medicine just came out of my own interests. That’s also kind of an autobiographical story. My maternal grandmother became a nurse because she was trained by the United States military during World War II and my paternal grandmother lost five of her siblings to disease. From my own family history I see very much the impact of medicine both in terms of loss of dear family members and in terms of the professionalization of women and the granting of new professional opportunities. It just so happens that my first book, which is an open-access free downloadable ePub online, is about the history of women’s place in the medical professions in China during the war with Japan. It’s called Intimate Communities: Wartime Healthcare and the Birth of Modern China. If any readers are interested you can just google “Nicole Barnes” and “intimate communities” and you’ll find your free download.
Currently, I’m starting research on the social, political, and cultural history of the use of night soil as farming fertilizer in China over the course of the late nineteenth and twentieth centuries. This is partly out of an interest in environmental degradation and the ongoing social prejudice against farming peoples and migrant workers in China today—-both of which are dire situations as I’m sure you know—- but also out of respect of the centuries of profound knowledge about how to combine animal husbandry and stewardship of the land to produce a dramatically productive agricultural output from a limited space of arable land. This is what Chinese farmers did for centuries—-they were the envy of farmers around the world for a long long time and the switch from the night soil economy to sewerage and disposal has actually been a source of deep environmental degradation, so I’m interested in the environmental humanities, medical hygiene, and sanitation aspects of that story as well as the social impact in terms of the treatment of rural people in whether we see them as a source of dirt or is a source of illustrious knowledge that has been held in Chinese culture for a long time. So it’s a project that has many strands.
That’s a great question and there’s two main ways I’d like to respond. First, it’s important to learn the specificity of medicalized racism against Asian Americans on U.S. soil, but also specifically Chinese immigrants back in the beginning of the twentieth century during a bubonic plague pandemic that began in southwestern China and made its way to Hong Kong. Because Hong Kong at the time was the primary port out of China due to its status as a British colony, the plague then made its way around the world and came to the Americas in the very late 19th century and led to the ultimate burning of San Francisco and Hawaiian Honolulu Chinatowns, demonstrating the deep prejudice against Chinese in the United States.
So that was like a flashpoint, if you will, the literal use of fire to supposedly purify these neighborhoods, but also an illustration of just how profound the racism against the Chinese has been since their arrival here in the United States. So for those of us who understand the history, when we started hearing about the conversation and the language that previous President Donald Trump was using, the recent spike in violence, and the horrible murders in Atlanta, they were deeply disturbing but not surprising because this anti-Chinese racism is so deep. Anti-Asian racism in general in the United States tends to ebb and flow, but I would argue that it never goes away despite these model minority conversations and the idea of Asians as an exception to U.S. racism. That sentiment is always present. The xenophobia and the average American’s fear / exoticization / obsession / attraction to things Asian and seeing them as exotic, strange, foreign and weird—-that has just always been a really profound part of U.S. culture and there’s a lot of lack of understanding that can come out into the open at times when a major Asian country is no longer the close friend but now is perceived as an enemy.
So you know, it really began not even with COVID, but with Trump’s trade war with China. I frequently traveled to China prior to COVID to do teaching for the Fuqua School of Business here at Duke. I did a trip to China during that time with business students, and the ones living and working in China at the time said as soon as the trade war started, they had a different feeling with their Chinese colleagues, and that the politics between the Xi and Trump administrations immediately entered their interpersonal relationships. I would say over the long-term, Sino-U.S. relations are always on this dime—- this tiny thin dime and it flips from friend to foe back and forth—- and it actually does enter interpersonal relationships in deeply troubling ways, so that thread is always there. So that’s one thing that we can use to respond to the most recent exacerbation of that kind of animosity—- with deeper awareness and knowledge of history.
And of course, early on in Asian American immigration history, there were a lot of Caucasians who would go see Chinese herbalists. That was not only a space of animosity but also of friendship and mutual understanding and respect so that’s another trend and another aspect of that history that bears attention.
What history and the humanities can bring to this event and to the problems of today is more global. It does not have to do with the specificity of the history of medicine, but more with the skills that a historian brings to bear on the world. When you are trying to do your historical analysis and recount histories, you have to do everything in your power to enter into the actual mindset and the way of being of a historical personage in order to understand their world, recreate their reality, and interpret and understand the sources that they leave behind—- the written records of court cases, personal letters, government documents, or newspaper accounts. That ability to practice entering in and stepping into the shoes of another individual is a profound skill that you can use in any other life setting because if you are constantly exercising your ability to think about something not from an egoistic, “me”-centric space, but from a position of trying to understand the other, that will make you much more empathetic, much more able to analyze any given situation from a variety of viewpoints, and therefore more flexible in responding to any kind of challenge. And that’s really what I think history as an academic discipline brings to the world.
Given the very long history of medicalized racism against the Chinese and Asians here in this country, any kind of hesitancy to accept a state-issued vaccine is something that I think should be understandable on the part of Asians in the U.S, even if they are U.S. citizens. Another thing that I think is important to bear in mind is that Chinese medicine and Chinese medical theories and ideas about health and illness in the body are distinct from a biomedical vaccine-centric and technology-centric approach, and we should really preserve respect for Chinese medical ways of being when we consider the issue of vaccine hesitancy.
I’m also just very glad to hear you use that language of hesitancy, because the most important and fundamental thing to keep in mind is that we will not be able to walk someone from vaccine hesitancy to acceptance if we don’t enter those conversations with an open mind and a willingness to listen much more than speak—-to listen and be receptive rather than coming in with a judgemental mindset.
In terms of access, in the field of Asian American history and Asian American studies, most recently in the last 5-10 years, there’s been a shift toward questioning the discourse of the model minority and challenging the ways that this image of Asian-Americans solidifies this idea that all Asian immigrants in the U.S. are upper-middle-class, people of wealth, means, and higher education. It also allows us to rewrite the history and the current realities in more complex ways that give attention to people of lower socioeconomic status, people who immigrated to other parts of the Americas and other parts of the world. After we put all of that into conversation, when we see that in a more complex light, then we can understand that in the Asian American community there are problems of access. Where are the poor and working-class Asian Americans? Where are the ones who have not had access to education to learn more English in order to understand all of the attributes of this foreign government and the public health information that is out there?
Even speaking as a historian of medicine who would self-describe as pro-vaccine and was very willing to get the vaccine, even I have had hesitancy after hearing the news about AstraZeneca, so I can completely understand how someone who is only hearing snippets here and there from some news sources or only hearing through word of mouth about resistance and hesitancy versus any kind of pro-vaccine sentiment.
It’s natural to understand that people would be hesitant. And then do they have a local vaccine center that they can access and can get to outside of their working hours? Or do they have an employer that’s going to give them some time off work to go to the vaccine center? All of these are really important questions. And I’ll just put a footnote there as well, that this is another place where the humanities and social sciences have something very important to offer, because we’re learning right now in a very poignant and powerful way, that it’s not just a matter of having the vaccine available. Being able to do all of that rapid scientific work was unbelievable and really unprecedented in all of human history—-to have multiple vaccines in such a short time period. It is phenomenally amazing and yet it’s still not enough, because if we cannot get the public information out there, if we cannot help convince people to be willing to have this put into their bodies, we are not going to be able to actually put that vaccine to use. So we need a broadband approach, if you will, that includes all kinds of sources of intelligence and ways of dealing with human beings to make this really work.
In traditional Chinese medicine, the core of it is really self care and preventative medicine. It’s making sure that you don’t get sick by keeping your own internal body very strong and your qi (life force) very strong. Qi is really just life force—- it’s that which expires or moves out of your physical body at the point of death and moves into your body at the point of conception. Keeping qi strong and keeping your whole body in balance through a good balanced diet, eating in accordance to the seasons at the right time, keeping your sleep schedule in accordance with the movements of the heavenly bodies like the sun and the moon, and of course sufficient sleep but also at the right time. Times are very important in Chinese medicine—- that’s a whole ‘nother topic that we don’t have time to go into—-but timing of illness onset, symptom presentation, and of self-care according your body to the times of the cosmos, all of that is essential and the core of Chinese medicine.
If you do all of these things, you cultivate your body and care for yourself, then ideally you have a lot of strength and resistance to any kind of pathogens or xie qi (pathogenic qi) that could attack your body. I could easily see some person who adheres very closely to a traditional Chinese medicine approach to health and illness feeling like the COVID virus is a form of xie qi and can attack my body, but if I strengthen my own body’s defenses and take herbal remedies that strengthen my respiratory system, then I am less worried about this virus because I know that I am going out into the world with this protection. Maybe I would also be willing to wear a face mask—-let’s not forget that face mask usage across China, and across Asia in general, is much more common and normalized than here in the United States. People do it for air quality issues, you know, if you’re riding a moped through polluted city streets, if you yourself are ill and you’re trying to prevent viruses and bacteria from invading, or just in response to the SARS epidemic of 2003.
Mask wearing has been normalized, so if people are willing to wear a face mask and they’re taking herbal remedies to strengthen their respiratory system and doing everything else in the suite of things that they know how to do, learned generally from parents, grandparents, and wider culture, to care for their bodies, I could completely understand someone who says “No, I don’t need to take the vaccine.”
There’s also another kind of aspect to this, which is that the vaccine could be conceived as the nuclear arsenal version of responding to this virus, whereas self-care, diet, sleep, and moderating everything about your body and its environment is a more gentle approach. That is often a point of contention between a Chinese medical etiology and a biomedical etiology. The other common way of thinking about that is antibiotics. A Chinese doctor might say, “Stop taking this antibiotic when you feel better because we know that the antibiotic destroys not only the bad bacteria but also the good ones, so we don’t want you to keep destroying yourself with that,” and of course that leads to antibiotic resistance and is an anathema in the biomedical community.
This really just comes from the different understandings of what health is about. In one world, it’s about balance and you don’t want to attack your body too much, and then in the other, it’s about bringing out the biggest arsenal against this danger.
From what I know sitting here in the U.S, I think in general I am very impressed and happy with what the mainland Chinese government has done with COVID to control it. Of course I am aware of and also concerned about the ways in which the Xi administration has used it as a pretext to advance and promote using artificial intelligence to track people’s movements and getting complete biopolitical control of people across the country. That is very much an issue of deep and profound concern.
But I think overall, if we’re going to talk about public health in general, China has done a remarkable job of controlling this pandemic. Yes, of course it did originate from Wuhan and now most recently even the Biden administration gave a nod to this theory that maybe it was something created in a laboratory and deliberately released or deliberately created in the laboratory and accidentally released.
I don’t personally give much credence to that. That, to me currently with the absence of real information, lives in the world of conspiracy theory, but a respiratory illness was bound to get out of a massive city, but I would challenge one to imagine a situation where in the city of such population density, any other country or governmental system would not have been able to control it as well and as efficiently as China did.
There were a lot of ways that they did that very cleverly. The universal enforcement of masking and quarantine, and yes, the tracking of people who tested positive, to ensure that they were observing quarantine and not moving out and infecting others. The use of forehead scanning for temperature, observation on busy street corners and making sure everyone had the face mask on, and now most recently not allowing people who have not received the vaccine to buy train tickets and move about freely. I mean I actually would like it if the U.S. government did some of these things to actually force people to show proof of vaccination, not just say “Ok, the CDC says we can stop wearing facemasks.” So now I, a US citizen, don’t know if the people who are unmasked and moving about have actually gotten the vaccine or if it’s just because they never wanted to wear masks. I think that’s going to lead to a long-term challenge here in the United States, whereas in China they have much deeper control. And then of course, as I previously mentioned, the normalization of face masks, but also other things that are less talked about like the building of large quarantine hospitals. Positive COVID cases in Wuhan early on were put into these hospitals, but they were with other COVID patients, so they were not forced into isolation. In the U.S., it’s all been isolation, stay-at-home, early on they were saying don’t even talk to people in your family. If someone gets sick, you isolate them in one single room. This is when we thought that maybe it could be transmitted by fomites, so anything a sick person touched could be a source of disease. Just having your spouse or your child serve food to you at the door and leave—-that is extreme isolation and that’s not good for a person’s sense of overall health. Again, going back to the Chinese medical idea of health as an overall holistic kind of health.
What I’ve seen reported about these group COVID isolation hospitals, is that the people there were happy to be able to do little activities with each other and not be in complete isolation. Yes, they might have been away from their family members, but they were interacting with other COVID patients and able to live a social life throughout that period as well, which I think is a distinctive Chinese approach to it that makes a lot of sense.
I: Thank you so much again for all your time Dr. Barnes. This has been such a productive conversation. I think that there’s a lot to unpack from what you’ve shared with us today regarding not only what’s been going on here in the States but also what has happened in China with COVID-19. You’ve demonstrated the value of history and the humanistic disciplines in contributing to understanding of the world and how we approach the problems and issues that we face in our modern society and I wanted to thank you again for providing such valuable knowledge and sharing that with all of us.
B: Thank you for having me, it’s my pleasure!
I: Thanks everyone again for tuning in!

Alexander Nicholas
Alexander Nicholas
Steering Committee Member @ PAQ (Philly Asian and Queer)
Key Words: LGBTQIA+ community, community based organization, mental health
I: Welcome everyone to the APAMSA NHAAPI Health Issues Interview series, where we’ll be interviewing researchers, policymakers, community-based organizations, and other experts on health-related topics that affect the NHAAPI community. My name is Grant Wen and I’m the health advocacy director at APAMSA National.
For this interview, I would like to welcome Alexander Nicholas from Philadelphia, Asian and Queer, also known as PAQ. PAQ is a volunteer social organization that strives to engage queer Asian and Pacific Islander folks within the Greater Philadelphia area. Through a range of advocacy, social, and supportive programming, PAQ commits to building and uniting their collective voices as queer AANHPI communities. Alexander Nicholas, pronouns they/them, is a steering committee member of PAQ and currently at a master’s program of social work at Widener University. So without further ado, let’s welcome Alexander.
My name is Alex or Alexander, and I’m a second generation Filipinx, trans masculine, non binary person. I became involved with PAQ two or three years ago. And our organization has a range of programming. I’m mostly involved with our afternoon tea and discussion groups, where we discuss various topics related to the queer NHAAPI community. Before COVID, we also had food tours, where we would all get together and go to various NHAAPI owned restaurants to support them. And currently, in COVID, we’ve moved almost completely to online at this point. We are trying to get back to in person events. We recently had a drag night. And right now we have a Discord server, facebook group, and instagram handle.
I think because of the pandemic, and the hyper visibility that the AANHPI community was suddenly facing, a lot of our topics of discussion shifted to more of dealing with our mental health and how to weather a new surge of racism against us. Because a lot of our community was based on feeling like we didn’t have visibility within the queer community, as Asians and Pacific Islanders. And so now it’s like, okay, well, we can’t really separate these identities. So how are we being affected by racism right now?
In addition, before the pandemic, we as an organization had been talking about trying to put together a queer AANHPI conference. And just something small, where we could have various workshops and speakers, to try to grow the community and connect with other organizations in Philly. But then COVID happened. So those plans were put on hold. But other than that, we also partner with Laneway Community Center and do our fundraising through them. And I think one of our goals j has been to start a queer AAPI Scholarship Fund.
Lastly, for those of you who don’t know, the Laneway Community Center is located in Center City, Philadelphia. And it is, I think, one of the older or oldest queer community centers in the city. I’m not quite sure if they’re open right now, but we also used to hold our afternoon tea and discussions there.
There have definitely been new challenges after COVID. In the past, community work was 90% in-person events, like gatherings at community centers where individuals could share food or celebrate festivals and special holidays together. But due to COVID, people couldn’t gather and don’t feel comfortable doing so. So that was a huge challenge, especially for some of our community members, as the majority of clients we serve are the elderly with limited English proficiency, and really limited knowledge and even access to internet and digital devices.
COVID really changed everything for our organization also. First, we couldn’t work in our office building, so we had to work from home.Second of all, we had to transition events and projects to digital platforms, and to do so, the initial steps we took were to do digital literacy programs for the seniors in the communities that we serve. I know that some of our partners called the seniors individually and gave them instructions on how to use Zoom, how to create an account, etc. And then they went into health education and even social gathering through zoom and other digital platforms. So that was really new to us. But surprisingly, they all adapted to the digital world fairly quickly. The seniors seemed to become very familiar with the platform, and they really enjoyed talking to each other. So that’s really going smoothly for now, but with things slowly transitioning back to reopening, I’m sure there’s going to be new challenges, and we will see how we can adapt to any new situations.
We also have been supporting local businesses since the pandemic. For example, we ordered 1000s of masks from a local Vietnamese shop. That’s one of the ways that we’re supporting the local community. We also collaborated with the local businesses in Chicago, where they helped us distribute the resources that we created, such as handouts with in-language materials and resources for local communities.
Right after the pandemic hit, everyone—-but especially the communities we serve (elders with limited English proficiency)—- had been isolated at home. So we collaborated with APAMSA to create a student ambassador program for students to call seniors who felt isolated to make sure they felt supported enough to meet their physical and mental needs. Especially after the anti-Asian violence, there was a huge increase in mental health needs for the coming from the elders in our communities along with even more hesitancy in going out. We’ve received some good feedback, especially with the program that we’re doing with APAMSA. Seniors across the country appreciated the company and the conversations they had and also the students helping them process COVID information and also the vaccine.
With our community, a lot of the health issues that we were dealing with, via our organization, were mostly related to mental health and finding community and reducing isolation. The queer AANHPI community also still deals with AIDS/HIV, and especially as immigrants, there can be a language barrier to accessing services for that. And a lot of our steering committee members happen to be social workers, so we are personally very involved with trying to help with those disparities.
I would describe PAQ as very grassroots. It involves programming by and for the community. The kind of barrier to entry to becoming a steering committee member is quite low, I think, compared to other organizations, which I really like. And so when we have programming, it was very much a loop of feedback of just like, “Oh, well, I personally need community in this way. Can we work together to try to make that happen? In terms of our members, I think it’s a mix of first and second generation immigrants. Among both steering committee members and members who are not part of our steering committee, we have a wide range of NHAAPI experiences.
There has been a lot of discussion around feeling trapped and paralyzed around how to move through the world when you’re dealing with queer phobia and transphobia, and anti Asian racism. Because of the pandemic, a lot of people also moved back in with their families. Many times, members of the AAPI community will choose not to come out to their families, because it’s more important to maintain the relationship dynamic of the family. But when you’re stuck at home, it becomes harder and harder sometimes to maintain that balance. But if you go outside, you risk anti Asian violence. And a lot of people have just been struggling with that balance and trying to engage with coping skills.
Since I’m mostly involved with our afternoon tea and discussion groups, this topic of discussion has come up really frequently—-of people needing mental health support, or just community support. And being in a space where everybody has some kind of base level of similarity can really help you feel seen, even if you are talking directly about the specific struggles with COVID and anti-Asian violence.
There’s also definitely a shortage of therapists in general. One of the main factors of me choosing to change careers, from animation into social work, was the lack of queer therapists. And we are out there, but everybody’s rosters are always full. And so we can always use more mental health professionals, not just for the queer AANHPI community, but for the general population as well.
Depending on who you talk to, vaccine hesitancy will range within the community. I think there can be a misperception that marginalized communities are monoliths. So I think there can definitely be more work done addressing language barriers and science communication.
Within the community, a lot of people just don’t know the science of it. So I think that’s part of why there is some vaccine hesitancy. I think there is also some form of linguistic barrier. And unless you are connected with the medical community, or kind of in tangent with it, then it’s difficult to feel like the information is for you. But there also is the issue of Asians not being represented very well in data collected for vaccines for vaccination rates.
I think just spread the word. There is more than enough space for more members. And there’s really a lot of monthly opportunities to get involved. We have our Facebook group, a Facebook page, an Instagram page, and our mailing list is very comprehensive and covers our events as well as the communities that might be relevant.
I: Before we end this interview, I was wondering if you had any kind of major takeaways that you wanted listeners to come away with.
A: I think I would like listeners to remember that our mental health is also connected to our physical health. And that having a strong community and network density of your community connections can really help maintain good health.
I: Thank you so much, again for sharing with us! It was a pleasure to talk to you today.